Laika Gokcekus1 ![]() ,
Arijana Mestrovic2,
Bilgen Basgut1
,
Arijana Mestrovic2,
Bilgen Basgut1
For correspondence:- Laika Gokcekus Email: laika_gokcekus@yahoo.co.uk Tel:+905428659343
Received: 9 June 2016 Accepted: 19 September 2016 Published: 31 October 2016
Citation: Gokcekus L, Mestrovic A, Basgut B. Pharmacist intervention in drug-related problems for patients with cardiovascular diseases in selected community pharmacies in Northern Cyprus. Trop J Pharm Res 2016; 15(10):2275-2281 doi: 10.4314/tjpr.v15i10.29
© 2016 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To investigate the role of the community pharmacist in identifying, preventing and resolving drug related problems (DRPs) encountered by patients, with particular emphasis on cardiovascular drugs in community pharmacies in Northern Cyprus, Turkey.
Methods: A prospective observational study for the assessment of DRPs and pharmacist interventions in cardiovascular diseases patients was conducted over a period of four months at four community pharmacies in North Cyprus. Interventions were then evaluated and classified using the Pharmaceutical Care Network Europe PCNE DRP classification tool V6.2.
Results: It was determined that 63 % of patients requiring intervention had problems related to drug use linked to existing diseases. The most common cause of DRPs was adverse drug reactions (ADR, 54 %), while the most common reason for DRPs in this group, ‘Others’ (54 %), was significantly (p < 0.0001); ‘Others’ included compliance problems and unclassified complaints. All patients were counseled. Sixty three percent of the encountered DRPs were completely resolved after intervention; the outcome of the intervention was unknown in 36 % of the patients, but the problem could not be solved in only 1 %.
Conclusion: Adverse drug reactions are the most common DRPs in patients with cardiovascular disease. Pharmacist intervention is effective in reducing the level of DRPs.
Introduction
Drug related problem (DRP) is defined as ‘an event or circumstance involving drug treatment that interferes with the patient acquiring an optimum outcome of the treatment’. This definition includes medication errors encountered in the period from prescribing to dispensing, implementation of the medication and also adverse drug reactions (ADR) [1]. Medication errors lead to irrational drug use which is related with improper drug selection, incorrect dose and formulation.
When providing pharmaceutical care, drug related problems identification is essential. It is important not to confuse medication error (ME) with the DRP. ME refers to the mistakes in the process that could lead to problems, while DRP can originate during prescribing, dispensing or taking/administering medicines. Even though it is not always noticed, drug use problems by the patient are probably the most frequent ones. There are several classifications for drug related problem, but in this study the classification of the Pharmaceutical Care Network Europe (PCNE) is used to clarify the concepts [2]. Both physicians and pharmacists are responsible for the medication errors in irrational drug use, while patient adherence is also very important in terms of accurately maintaining treatment. One of the other major reasons for DRPs is the tendency of the patient to use OTC medicine without consulting a pharmacist [3]. To obtain a safe and effective use of medicines collaborative work within all health care professionals is crucial. Both in the community and in hospitals, pharmacists are critical health care professionals to ensure the appropriate use of medicines [4].
The pharmacist is a substantial health care professional in the identification of a DRP, in the correct implementation of rational drug use principles by giving drug-related consultancy services, and in development and improvement of pharmaceutical care services by observing the patient during the treatment process.
Cardiovascular diseases (CVD) are still the first cause of morbidity and mortality according to the World Health Organization (WHO) [5]. It is well known that the incidence of polypharmacy has increased in patients with CVD because of the associated co-morbidities. Polypharmacy is one of the most important underlying causes of DRPs during therapy. In studies related to the determination of DRPs, the frequency of DRPs has been reported to be high in these patients [6,7].
The aim of this study was to investigate the role of the community pharmacist in identifying, preventing and resolving DRPs in patients, with CVD in North Cyprus using the PCNE classification system.
Methods
Study design
It is a prospective, cross-sectional observational study for the determination of DRPs, causes of them, possible interventions and its outcome in community pharmacy. This study was carried out over a period of four months between March and June 2015. It has been performed in 4 community pharmacies in North Cyprus. 100 patients with hypertension were randomly selected for this study. PCNE V6.2 form was used for the identification and classification of the DRPs. DRPs were identified by evaluating treatment effectiveness, adverse reactions, treatment costs, others such as patient therapy dissatisfaction or unclear problem/complaint. The form was used to collect data/information from each patient. Confidentiality of the information used in this study was maintained. Patient name, or ID, name of the prescriber, and name of the pharmacist who did the intervention were not disclosed. This study was approved by the Ethical Committee of the Cyprus Turkish Pharmacists Association.
Data analysis
Data were expressed as a percentage of the total number of patients included in the study.
Statistical analysis was performed using SPSS (version 19.0). Chi-square test was used to test for significant differences within the groups, which are categorized in the PCNE form such as the type and the cause of the problem, intervention and outcome. Correlation between the type and the causes of the problem, intervention or outcome were determined by Spearman correlation analysis. P < 0.05 was considered as statistically significant.
Results
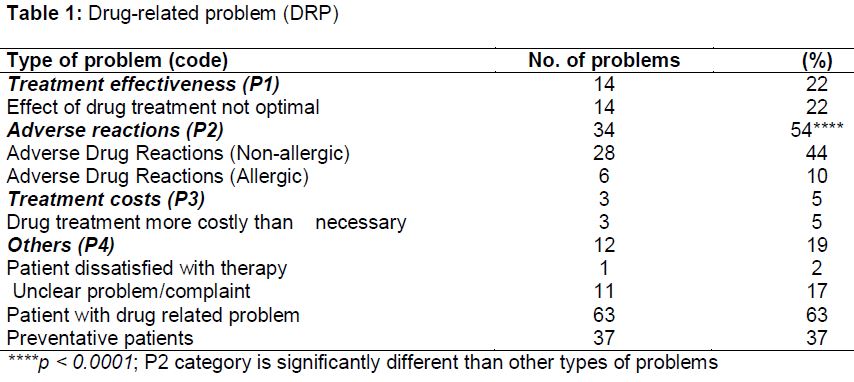
Out of the 100 patients used in this study, 80 DRPs were found, and more than one DRP was detected at a time in 20 patients. It was determined that 63 % of patients requiring intervention had problems related to drug use in relation to their existing diseases. It was observed that the remaining 37 % of the patients did not have any DRP but the condition of the existing disease or co-morbidity would worsen if there were no intervention. These interventions were then carried out and evaluated as preventative. Fifty four percent of these problems were identified as adverse drug reaction and this was found statistically significant (p < 0.0001). While treatment in lack of effectiveness was recorded as 22 % of the different types of DRPs, 19 % were classified as 'Others' which included compliance problems and unclassified complaints. We encountered cost-related problems in only 3 patients ().
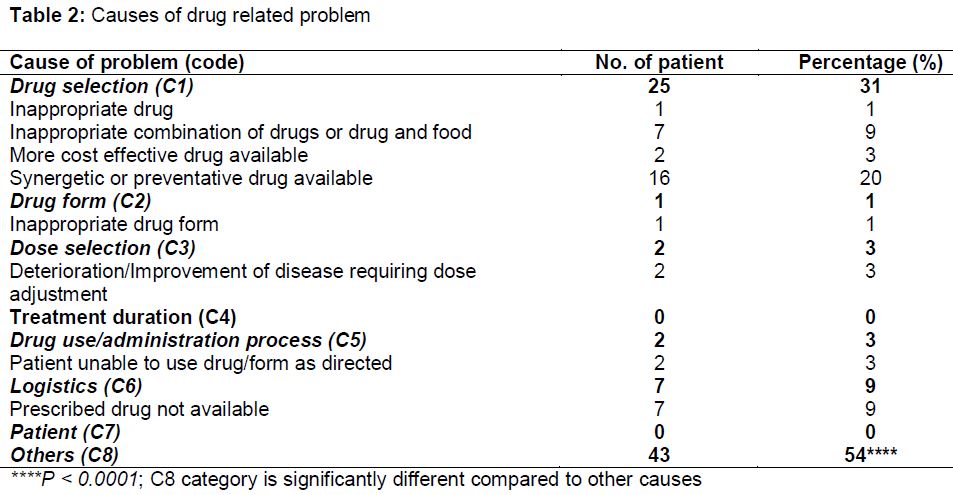
When the reasons for DRPs were examined, 54 % were identified as 'Others'. The need for synergistic/preventive medicine (20 %), inappropriate drug combination (9 %) and the absence of the drug to be administered in the North Cyprus drug market (9 %) were the other major reasons for DRPs. Patients suffering from improper drug administration, no follow up on whether the disease had progressed or worsened, being prescribed inappropriate drugs or in an inappropriate form were among other DRPs encountered. Duration of treatment and DRP related to the patient were not encountered ().
Based on the causes of the DRPs, ‘Others’ (C8) category was higher than the other causes significantly, and include intolerable side effects, inadequate blood pressure control, compliance problems, insufficient knowledge on drug usage.
Interventions were done by evaluating patient’s laboratory values according to the drugs side-effect profiles, recommending OTC food supplements according to laboratory values and finally convincing patients about the efficacy of their treatment.
In the PCNE classification, the types of interventions were given at five different categories which include; no intervention, intervention at prescriber level, intervention at the patient level, intervention at drug level, and ‘Others’.
“Patient counseling” applied to all the patients who come to the pharmacy as an intervention at patient level at least once. This was the significantly (p < 0.0001) highest category as compared to the other types of intervention.
Recommendations of life-style changes, quitting smoking, salt/sugar intake reduction and exercise were given to the patients with hypertension or co-morbidity for the well-being and improving the quality of life.
Only 6 patients received medical intervention at prescriber level. The prescriber was contacted after a problem was detected during dispensing. The problem was resolved and after confirmation from the physician, the patients were informed about the changes to their treatments.
Forty five percent of patients received intervention at the drug level. Fifty eight percent of these drugs were changed by their physician as the outcome of the intervention performed. A new drug was initiated in 19 % of the patients, while drug use instructions were changed in 12 % of the patients. The dose of the drug was changed in 8 %, drug was stopped in 4 % and formulation of drug was not changed in any of the patients.
‘Other’ intervention category constituted 62 % of the patients. In this category, tablet color was changed in 8 patients, usage of OTC (resveratrol, CoQ10, etc.) was recommended in 8, blood pressure was monitored before additional dose in 2, instructions were changed in 2 and cheaper generic drug was recommended in one patient.
All the patients received patient counseling. 50 % of these patients received only drug counseling, while 48 % of them needed referring to the prescriber besides patient counseling. Whereas it was attempted to implement drug counseling, referral to a physician and the principles of rational drug use by getting in contact with the family members/nurse in order to provide the most efficient and reliable benefits of drug treatment in only 2 % of the patient.
Sixty three percent of DRPs were completely resolved as an outcome of interventions performed. The outcome of the intervention was unknown in 36 % of the patients, and it was recorded that the problem could not be solved in only 1 % of the patients.
There were positive strong and significant correlation between treatment effectiveness (P1) and drug selection (C1); the adverse drug reactions (P2) and other (C8) category; or the other category (P4) and logistics (C6) using the Spearman's correlation analysis.
Discussion
DRPs are events involving drug therapy that actually or potentially interferes with desired health outcome negatively [8]. Contraindications, interactions, ADR and ineffective treatments are examples of DRPs. Prescribing errors, compliance problems and ADRs are among the causes for these problems. Polypharmacy, co-morbidity, aging, non-compliance, lack of coordination between different physicians all may increase the risk of DRPs [9]. Accurate identification and classification of the DRP prior to solution by the pharmacist is very important.
The latest version of the PCNE system V6.2, was used in this study because it was specified in many studies that the PCNE system is a convenient system for the classification of DRPs in clinical pharmacy services [10,11].
It has been reported in studies conducted in relation to the determination of DRPs that the majority of these are with CV drugs [6-7,9,12]. In relation to this, comprehensive drug treatments should be considered in patients with CVD in order to prevent potential/possible DRPs that cause adverse clinical outcomes. Although DRPs are frequently encountered in CVD, there is no enough information in the literature about their types and what causes them. In this study, DRP in patients with cardiovascular diseases were aimed to be examined in North Cyprus.
In a study conducted in Khoula Hospital in out-patients since 2009, documentation of pharmaceutical intervention was initiated and patient intervention during this period was performed by the pharmacist or pharmacist’s assistant [13]. In all of our interventions, one to one patient counseling was performed. Consultation with the physician was performed by 48 %, while intervention was carried out with the patients and patients' relatives and the physician was contacted in the ratio of 2 %. In the study performed by Rahbi et al, interventions were performed in written form at the hospital pharmacy. The pharmacists apply the errors detected by submitting them to their physician again by adding their impressions to the prescription in handwriting, and in return the physician was asked to correct any conditions that were not clear or related to the drug [13]. Sometimes interventions were performed via phone calls to the physician, and in 6 % of the patients in our study, attempts were made to contact the physician immediately in order to resolve the DRP. In some cases, the problem was identified and the patient was referred to their physician to resolve the problem. Unfortunately, it was not possible to follow the intervention outcomes of all of the patients referred to the physician. In addition, the absence of proper patient-physician-pharmacist information/communication network in North Cyprus health care system is among the reasons for that.
Prescription errors are among the most common reasons for DRPs. It has been shown that DRPs cover 5 % of all hospitalizations, they are encountered in 10 to 20 % during hospitalization and cause prolonged hospitalization in 7 to 9 % [14]. In a study performed by Javedh Sharef et al in 2014, drug interactions (49 %) and adverse drug effects (19 %) were found to be the first two causes of DRPs [15]. In another study, ADR were found to be the most common DRP (41.5 %). This finding is comparable with our study. Khan et al [10] reported non-effective treatment ratio as 22.4 %, which is similar to what was obtained in this study. It was observed that problems related to the cost was lower (3 %) compared to other/previous study (20.4 %).
In a study conducted in India, it was observed that improper dosing and improper drug selection were frequently encountered among the causes of DRPs and it was thought that standard treatment protocols and each hospital having their own treatment patterns were the causes [16]. Although improper dose selection was the most common cause of DRPs (25.4 %) in the study performed by Prassana et al [17], in another study, it was reported as inability to use/to implement the drug. While drug selection is 31 % in our study, the reasons connected with the implementation of the drug is low (3 %). Although issues related to dosing were the most significant (42.2 %) in the reasons for DRPs in the study conducted by Khan and Ahmad in 2014, drug level interventions were the most utilized interventions (50.9 %) followed by physician level (40.4 %). As a result of interventions, problems were completely resolved in 86.3 % of patients, partially resolved in 6.8 % of patients and in 6.8 % of patients the response was unknown [10]. However, we did not encounter "partially resolved" condition in our study. Although improper dosing and drug selection were not significantly high in our study, lack of the standard treatment protocols and each hospital/physician having their own treatment choices may have contributed to such in the study. It is thought that these differences regarding not determining the reasons arise from the use of different systems in classification.
The determination and resolving of DRPs by the pharmacists is possible as a result of accurate and timely intervention. The interventions offered to physicians by clinical pharmacists have the highest acceptance in terms of the resolution and the prevention of DRPs. 41-96 % acceptance has been reported [18-21]. It was unfortunately not possible to compare this to our study, because the case of not knowing the outcome of the interventions performed were very high.
Although the community pharmacists are not exactly the same as hospital pharmacy in North Cyprus, the interventions were performed directly on the patient. Ultimately, it was observed that the patient-pharmacist-physician network is not adequate; patient information can only be obtained through direct contact with the patient/patient relatives/the physician and its reliability is controversial.
In another study performed by Douchette et al, the acceptance rate of interventions is still low (47 %) and the reason for this has been described as the pharmacist had difficulties in accessing the patient's specific information and also the form of interventions offered by pharmacists were in the form of written reactive disclosures [20]. The deficiencies in the North Cyprus health system, the difficulties in accessing patient drug/treatment application form information have also limited our study.
Another important issue in terms of DRPs is treatment cost. A study that examines the relationship between the cost of treatment and pharmacist intervention is needed. This relationship could also not be examined in our study because we do not have information on the financial condition of the patient and/or the cost of the treatment to the government, and the lack of pharmacy automation systems. A study for the entire country to observe the effect of the government on health economy would be helpful.
Similar to the aforementioned studies, the outcomes of interventions performed on the patients in order to resolve the DRP, including mutual interventions with the physician, have always been positive in our study. Although patient counseling was carried out in 100 % of the patients, 63 % were resolved completely in the pharmacy or on a return visit after advice was given. The patients visited the pharmacy again to request the new form of the recommended treatment. However, the outcome of the intervention being unknown was very high (36 %). Because of the follow-up difficulties, it is not known whether the recommended intervention was utilized or not.
Similar to our study [12]; it has been suggested that it is because of follow-up difficulties in knowing to what extent the patients’ medical condition has been affected after the intervention following the discharge of the patient. While one of the major problems we encountered in our study was the direct request of the drugs by the majority of the patients or the physicians neglecting to write down the diagnosis while prescribing the medication, led us to be without knowledge of the patient's diagnosis. Among the main reasons behind this problem are lack of necessity to specify the diagnosis on the prescription in the existing North Cyprus health system, patients being able to obtain drugs without prescription, sometimes the person who the drug is dispensed is not the patient, lack of sufficient information about their disease and drug history.
Limitations of the study
The study has some limitations due to the fact that not all the necessary information was obtained from the patients, patients not willing to wait for detailed drug counseling, lack of adequate knowledge of patients’ treatment details, poor or no response by patients because counseling was still new at the time of the study.
Also, in some cases, prescriptions were collected by patient’s care providers/relatives, inadequate drug information system database, and that good pharmacy practice is based on the information given by patients/patient care providers, but not only the health care provider.
Conclusion
In North Cyprus, ADRs are the most common DRPs in patients with cardiovascular disease based on PCNE classification system. The results obtained from this study are important because it is the first in Turkey and North Cyprus for the identification of DRPs, and should guide future studies in this subject area. The role of the pharmacist in identifying, preventing and resolving DRPs is important in improving therapy outcomes.
Declarations
Acknowledgement
References
Archives


News Updates